

#1 Vaccines!
Vaccinations for COVID-19 began to roll out at the beginning of the year and we’ve worked hard to raise awareness and advocate for all our kids to be protected. We’re hoping shots for our littlest lobbyists and boosters for big kids will be available soon. Please keep doing all you can to protect yourself, your family, and all of us - wear a mask, get vaccinated and boosted as soon as you can! To learn more, visit vaccines.gov.
In the photo: Little Lobbyists Simon gets his COVID-19 vaccine!

#2 Virtual Meetings, Real Advocacy!
We love introducing legislators to our kids, and COVID didn’t change that. Like so many others, we took our work online and are continuing to make sure kids with complex medical needs and disabilities have a seat at the (virtual) table.
In the photo: Little Lobbyists Taryn and her mom Dawn meet with Senator Sinema and her Team.

#3 Congressional Testimony!
The American Rescue Plan included many provisions to help all our families, like the Child Tax Credit, funding for home and community based services for people with disabilities, and subsidies to make health insurance more affordable. Our Director of Communications, Laura LeBrun Hatcher, was invited to testify in the House of Representatives to explain why these provisions are so important, and why they must be made permanent.
In the photo: Little Lobbyists Simon’s mom and Director of Communications Laura LeBrun Hatcher provides testimony to the U.S. House of Representatives.

#4 Celebrating the Americans with Disabilities Act!
This year the ADA turned 31 and Little Lobbyists Executive Director Elena Hung was invited to a celebration marking the occasion in the White House Rose Garden. At the event, President Biden acknowledged that there is still much work needed to remove barriers to freedom and equality for Americans with disabilities and he affirmed his administration's commitment to advancing Disability Rights. Watch the ceremony here.
In the photo: The president surrounded by the Vice President, disability advocates, Speaker Pelosi and other leaders mark the anniversary of the ADA.

#5 Meeting with the Vice President!
Twice this year, Little Lobbyists had the opportunity to meet with Vice President Kamala Harris to represent our families and discuss what our children with complex medical needs and disabilities need to survive and thrive. Communications Director Laura LeBrun Hatcher joined the Vice President at an event celebrating the Affordable Care Act and Little Lobbyists Claire’s mom Jamie Davis Smith sat down with the Vice President at her own kitchen table to discuss the importance of caregiving. Read Jamie’s account of her experience here.
In the photo: Vice President Kamala Harris sitting at the kitchen table for a conversation on caregiving with Little Lobbyists Claire’s mom Jaime Davis Smith.
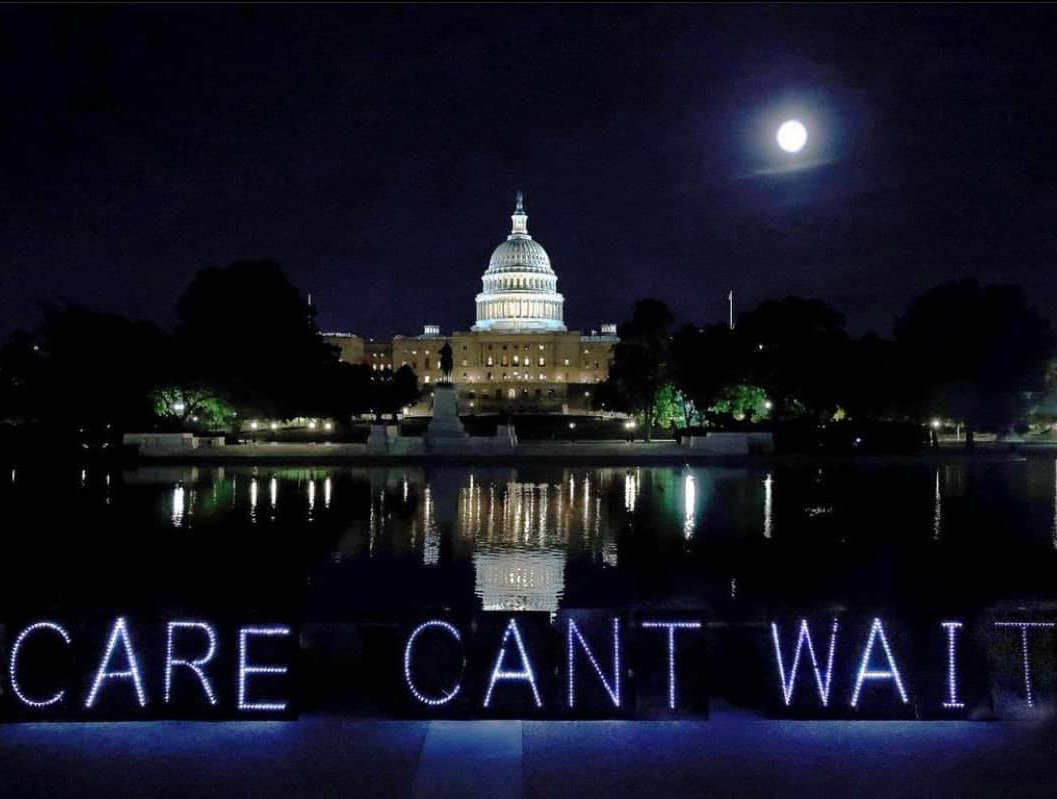
#6 Care Can’t Wait!
President Biden’s agenda calls for a major investment in our country’s infrastructure — including social spending on health care, education, and caregiving as part of the critical foundation our country must support to remain strong. The social infrastructure bill is called the Build Back Better Act. Working closely with Senator Casey and Representative Dingell, Little Lobbyists provided input on the policies and funding our loved ones with complex medical needs and disabilities need to thrive at home instead of being forced into dangerous institutions. For the past several months we’ve advocated alongside many other organizations to get this historic legislation passed because for our families ”Care Can’t Wait!” To learn more, visit www.littlelobbyists.org/carecantwait.
In the photo: Activists lit up the night with “Care Can’t Wait” signs in front of the Capitol following a 24 hour rally.

#7 Powerful Partnerships!
In a year full of historic challenges and opportunities, we worked collaboratively with several organizations to advocate for the passage of the Build Back Better Act including: the Arc, Be A Hero, the American Association of People with Disabilities, the Autistic Self Advocacy Network, Caring Across Generations, the Center for American Progress, MomsRising, the National Domestic Workers Alliance, SEIU, and many more. In addition, we partnered closely with Ady Barkan’s organization Be A Hero to help share our families’ stories about the importance of home and community based services on a national platform.
In the photo: Director of Community Engagement and Little Lobbyists Sara and Emma’s mom Stacy Staggs shared her family’s story nationally through our partnership with Be A Hero.

#8 A “mom to mom” conversation with a U.S. Senator!
Executive Director Elena Hung had a mom to mom conversation with Senator Maggie Hassan. Elena and the Senator were both led to national advocacy through their experience as parents and caregivers of disabled children. They discussed the importance of Medicaid home and community based services and the policies we need to ensure our children have the civil rights they deserve. Watch the video here.
In the photo: A screen shot from the video call between Senator Hassan and Little Lobbyists Xiomara’s mom and Executive Director Elena Hung.

#9 The Build Back Better Act passed the House!
The Build Back Better Act includes historic investments in home and community based services, access to health care, education, childcare, paid leave, lower drug costs, and more that our families need. Our Executive Director Elena Hung was invited to the White House with a small group of disability advocates to support the final push to the House vote. Our work to get this bill passed is far from over – the legislation is currently in the Senate and intense advocacy will be needed to get it over the finish line.
In the photo: Disability rights leaders, including our Executive Director Elena Hung, with a White House Associate Director beside the White House.

#10 Little Lobbyists are invited to the White House!
We work hard but also remember to take time to celebrate. At the invitation of the President and the First Lady, we spent some time viewing the beautiful holiday decor at the People’s House. Masks were worn and social distancing observed, but the lights shined just as bright. We appreciated the care taken by the Administration to ensure this year’s subdued holiday celebrations were as COVID safe as possible ahead of the Omicron surge.
In the photo: Members of the Little Lobbyists team, Elena Hung, Laura LeBrun Hatcher, and Jeneva Burroughs Stone stand in front of a stairway lit with candles leading to a festively decorated entrance to the White House before they tour the holiday decor.
In the coming year, Little Lobbyists will keep showing up to represent our families and make sure ALL kids with complex medical needs and disabilities have a seat at the table to inform the policies that affect them. To be a part of our ongoing advocacy, follow us on social media, share your story with us, and if you can, please consider donating to support our family-led and volunteer-powered work.
Wishing everyone a happy and healthy 2022!




















![Myka holding her vaccine card. [image description: A light-skinned girl with shoulder-length blond hair holds up her vaccination card. She is standing outside a chain drug store, with signs on its windows. She wears a striped t-shirt and denim shorts.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1634316674792-7G0UD6AOXK9W4CY42HF0/Myka+vaccine.jpeg)




![Kim’s sons Elijah (l) and Isaac (r). [image description: Two young boys with light skin stand closely together with their arms around each other. One wears a blue plaid shirt, the other a yellow t-shirt with the words “Wakanda Forever” and an image of Marvel Comics’ Black Panther.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1633014381552-N2JKFLPPH74EF7VXQ3VY/Kim+gould+Crawley+LL+blog.jpg)

![Art by Rob Stone, yarn on ceramic tile. [image description: Pieces of yarn (dark & light blue, light & dark green, red, orange, and yellow) have been dropped in tangled loops on a glossy white ceramic tile and glued into place.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1632413342229-TWA0JJKMYL8072SA9GL9/tempImagehuj8oU.png)
![Stock photo. [image description: A young boy (left) with pale skin wears a blue surgical face mask and yellow shirt and carries a royal blue backpack. He elbow-bumps a young girl (right) wearing an identical face mask who has pale skin and braided hair. She wears a blue-striped shirt and carries a pink backpack. The two stand in front of a school building.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1631199249508-Y6RIA546S6IZG9LM9CCK/iStock-school+masking.jpg)
![Elvina’s daughter Colby. [image description: A young woman with light-colored skin smiles at the camera; she is seated in a family kitchen. Her brown hair is pulled back from her face. She has braces on her teeth, and wears a gray hoodie.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1630597945352-WULI9QCTOR8W6JIF1PN9/colby+street.jpeg)
![Colby and Elvina. [image description: A black and white photo of a mother and daughter. The daughter, to the left, looks away from the camera, smiling. The mother looks directly at the camera.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1630597549860-42C9MVF2L0CM085WQ7LF/colby+and+elvina.jpeg)
![Little Lobbyist Simon Hatcher poses in front of the U.S. Supreme Court steps with his dog. [image description: A light-skinned disabled boy poses in his wheelchair in front of the white marble steps of the U.S. Supreme Court. The Court’s Corinthian columns and can be seen in the background. The boy holds the leash of his dog, a large curly white-haired breed whose long pink tongue is sticking out.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1629995605073-W50LQ3C7H77TD1OB986W/CA99AE73-C70E-4E49-A812-923AE242AEAF.jpeg)
![Disability activists Mia Ives-Rublee (center, Director of the Disability Justice Initiative at the Center for American Progress) and Elena Hung (right, Co-Founder of Little Lobbyists), two young disability activists, and two dogs in front of the U.S. Supreme Court. [image description: Left to right are seated on the pavement a large white curly-haired dog, a light-skinned boy with glasses, a large white short-haired dog, a light-tan skinned woman with short black hair, a light tan-skinned young girl with black pony tails, and a light-tan skinned woman with black hair pulled back. In the background is the facade of the U.S. Supreme Court.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1629995658029-MBBWSFMD04HYOUW6DZC0/7A43971F-1BA0-4FAF-9048-5E1A0EA19D9E_1_201_a.jpeg)
![Nine young Little Lobbyists pose on a tree-lined Washington D.C. street with the U.S. Capitol building in the background. [image description: Nine young children with various skin tones pose on a city street with varying shades of pavement (grey, dark red, tan). Some of the children are in adaptive strollers with medical equipment, others stand. They are all goofing off, adorably.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1629995731331-HX9HIZXF46GGX6F1W97D/F163048D-C5AA-4566-AD57-D770D4ED2E1E_1_201_a.jpeg)
![Rob and his disability rights button collection. [image description: A business card on a brown wood table shows a man with light skin sitting in a wheelchair on a grassy hill overlooking the city of Washington DC. He wears sunglasses and a Washington Nationals baseball hat. Four round advocacy pins are placed near the business card: “Meaningful Work Community Inclusion Transcen.org; Little Lobbyists (with their star child & heart logo), “Disability Rights are Civil Rights”; “Health Care Voter.”]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1629392376323-YJLJ8M57UYT1ROKXV9JP/1545B987-D7FF-4F3D-A8FB-D667CA4C46F1_1_201_a.jpeg)
![Rob at a recent state park outing. [A young man with light skin sits in his wheelchair in front of a colorful wall mural with a Maryland State Map, beneath which is written “Nothing is real until it is experienced.” There are also painted images of a turtle, a crab, and a squirrel visible.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1629392486726-9B3VHHALJYISRRKQ6HGP/3F034076-5A0C-4C6F-A79C-8834CE7C9D7A_1_201_a.jpeg)
![Payton (center) with her dad, Randal (left), and her mom, Kristen (right). [image description: A dark-skinned man in a navy blue shirt holds his daughter, who had tan skin and is wearing a pink dress and a pink and white hair bow. The girl’s mother, a white-skinned woman is to the right with long straight brown hair and glasses.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1628715929675-Q2WDGYTG8YAPT5XO07XZ/Payton+w+mom+%26+dad.JPG)
![Payton (right) with her dad (left). [image description: A dark-skinned man wearing a knit cap and brown plaid shirt holds his young daughter, who has tan skin and is wearing an aqua jacket. She is looking at bright stained-glass windows.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1628716165821-L2205KQJCXJHIPIRYKGR/Payton+%26+dad.JPG)
![Cailyn out in her community, assisted by a direct support aide. [image description: A young disabled teen wearing pink sunglasses and a bright pink outfit sits on an adapted red bike. An aide assists her moving through a sensory “tunnel” (an open pipework on which various objects are suspended).]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1626797835564-AMEE9ZT6H78F9Y80KLGX/jen+reese+LL+blog.jpg)


![Sandra Stein (r) with her husband Matt (l) and their son Ravi (center) [image description: A white man and white woman pose on either side of a young Black man seated in a wheelchair. All three wear t-shirts with the words, “Caregiving Is Infrastructure.”]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1626366477314-C9IT63KOWEBTYYNUHZXH/Sandra+Stein.jpg)
![Angela Carpenter Gildner [image description: a white-appearing woman with blond hair poses in a gray “Health Care Voter” t-shirt with a red cushion in the background]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1625069902659-PF7QBYZ96UN0A9JDEK0W/24hcvangelahq-4.jpeg)
![Graham and Margot [image description: a white-appearing brother and sister, each wearing t-shirt and shorts pose knee-deep in a lake with mountains in the distance on a sunny day]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1625070133101-2G93ZFC0BPKBTCO65WGO/IMG_8243.jpeg)
![Ron Carlson [image description: A white-appearing man speaks at a lectern with a microphone]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1624550950455-N0KN4HDRPN6SKZ07K9V7/Ron-Carlson-1030x579.jpg)
![A meeting of the Maryland Regional Direct Services Collaborative [image description: A large group of people sit at tables arranged in a square in a community college meeting room.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1624551140263-LE980FUOR10UQ8OPJEAA/Newsletter+-+November+VIP+Luncheon+Picture.JPG)
![Peter Witzler and his family. [image description: A white-appearing father, mother and two young boys pose with their black dog in a wooded area near a stream. All are smiling.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1624375996493-55HYNOP8MNBL1IZUECCV/Witlzer+family.jpg)
![Peter and Lisa with Jackson just before his first surgery at three-and-a-half months. [image description: Two white-appearing parents hold their infant son, who wears a Superman cape.]](https://images.squarespace-cdn.com/content/v1/59d8124080bd5eadd869b8b7/1624376089879-IVB3YENZKLIZ37EIGQ24/Witzler+right+before+1st+surgery.jpg)